This past Saturday, we hosted our June Kidney Cancer Support Group meeting. This month’s featured speaker was Helen Clark, RN, a clinical nurse educator at the Novartis healthcare group. Every other month I host and facilitate the Weill Cornell Kidney Cancer Support Group to provide a forum to come together, and to learn and talk about a wide-range of topics related to kidney cancer.
At our latest meeting, we discussed several subjects, including two oral medications commonly used in advanced kidney cancer treatment, Votrient (pazopanib) and Afinitor (everolimus). It was a lively conversation about how these medications work, how to cope with and manage common side effects, and how pharmaceutical companies can help with financial issues related to treatment. Additionally, we talked about the process for FDA approval, open clinical trials and other kidney cancer treatments Weill Cornell Medicine has to offer.
The purpose of our support group is to provide a community and outlet for patients and their families and friends, as well as resources and a safe space for sharing and addressing concerns. There is great power in connecting with others who have been there before, and often, it is fellow kidney patients and loved ones who can be the best source of support.
Dr. Molina, Host of the Weill Cornell Kidney Cancer Support Group
Thank you to everyone who came this month! We always like to see new and familiar faces and hope you’ll join us at our next meeting in September. Stay tuned for an update on the date, topic and featured speaker for this session.
One of the linear accelerators used to deliver stereotactic body radiation therapy (SBRT) for prostate cancer at Weill Cornell Medicine/NewYork-Presbyterian Hospital
Advances in radiation therapy have enabled physicians to deliver high doses of radiation treatment with extreme precision, shortening treatment duration and reducing exposure to normal organs. For men with localized prostate cancer that hasn’t spread outside the prostate gland, this has led to radiation treatments that can be completed within just five treatments.
Initially this approach was developed on the Cyberknife Radiosurgery Platform. Cyberknife radiosurgery doesn’t actually refer to a knife or traditional “surgery,” but rather a specific type of machine that delivers radiation. Now, this five-treatment radiation for prostate cancer can be delivered using many different types of radiation machines, and as a result has undergone a bit of a name change. We now refer to this treatment as “stereotactic body radiation” or SBRT for short.
There are multiple reasons to select SBRT as treatment for prostate cancer. First, it only requires a total of five treatments over the span of one to two weeks, in contrast to standard external beam radiotherapy, which requires nine weeks of daily treatments. Additionally, prostate cancer success rates from SBRT appear comparable to other treatment modalities based on monitoring for up to nine years post-treatment. These outcomes were recently reported at the 2016 American Society of Clinical Oncology (ASCO) Genitourinary meeting.
This retrospective study reflects the longest follow up monitoring to date and demonstrates local control of the cancer, with nine-year freedom from PSA failure (rise of 0.2 ng/ml above nadir) of 95% for low-risk patients, 89% for intermediate-risk patients, and 66% for high-risk patients (determined based on National Comprehensive Cancer Network risk criteria). In the study, toxicity from radiation was low, and the dose utilized was 7.0 – 7.25 Gy per fraction. In prostate SBRT, appropriate treatment dosing is critical as higher doses have been linked with unacceptably high rates of toxicity. At the level used in the study, patients reported some bowel and urinary side effects that lasted less than one year. Overall, this study suggests that increased radiation doses and additional hormonal therapy did not improve outcomes; however, prospective studies are ongoing.
There is now enough data regarding using SBRT for prostate cancer treatment that it is an accepted treatment regimen by the American Society of Radiation Oncology (ASTRO), and the National Comprehensive Cancer Network (NCCN) guidelines. However, these guidelines explicitly state that prostate SBRT should, when elected, be performed at a center with high-volume and expertise. The physicians at Weill Cornell Medicine and NewYork-Presbyterian are very experienced in delivering SBRT for localized prostate cancer and have published many articles on this approach and when it should be used.
We will soon be opening a randomized study looking at prostate SBRT in conjunction with rectal spacer versus endorectal balloon in an ongoing effort to refine our treatments. The rectal spacer is a gel, placed between the prostate and rectum. By displacing the rectum from the prostate, it reduces exposure of the rectal wall to radiation. The spacer degrades over a period of three months and has been shown to reduce toxicity in patients undergoing standard external beam radiation therapy. We hypothesize that there will be similar toxicity reduction after SBRT. An endorectal balloon is another way to reduce overall rectal wall dose, by pushing the posterior rectal wall away from the prostate during radiation treatment.
As data for prostate SBRT continues to mature, more individuals with low- and intermediate-risk prostate cancer will likely opt for this convenient and efficacious form of radiation over more protracted courses.
For men with metastatic prostate cancer that grows despite hormonal therapy (also referred to as castration-resistant prostate cancer), chemotherapy has been a mainstay. The class of chemotherapy that has consistently proved to improve survival for men with advanced prostate cancer is called “taxanes.”
Taxanes target microtubules, which are structures in cells that are involved in cell division, as well as the trafficking of important proteins. In prostate cancer, one of the main ways taxane chemotherapy works to kill the cancer cells involves blocking the movement of the androgen receptor (AR) along the microtubule “tracks” towards the cell nucleus, a mechanism we discovered here at Weill Cornell Medicine.
There are two taxanes FDA-approved to treat prostate cancer, docetaxel (brand name: Taxotere) and cabazitazel (brand name: Jevtana). While the drugs are similar, men whose tumors have grown despite taking one drug often respond to the other. The challenge for oncologists has been pinpointing when exactly to switch treatments.
This research came to be because we thought that we might be able to increase the number of men who respond to taxane chemotherapy with an early assessment and by changing the drug for those who have a sub-optimal response. Simply put, those with no response or only an initial minor response had their drug changed at a much earlier time point then standard practice. This resulted in a higher response rate for the patients in the study.
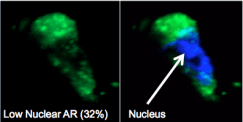
In the photos from a sub optimally responding patient, almost all of the androgen receptor (AR, labeled in green) is in the nucleus (indicated by the arrow which is overlayed in blue on the right), meaning that the taxane chemotherapy treatment was unable to block AR from moving to the nucleus and thus unable to kill the prostate cancer cells.
In addition, it’s very exciting that we can examine cancer cells from a simple blood test, a process also referred to as collecting circulating tumor cells or CTCs. This allows us to assess the ability of a drug to target the pathway in real time and to tell us whether there is a positive tumor response or resistance.
These circulating tumor cells provide an opportunity for real-time molecular analysis of taxane chemotherapy and at Weill Cornell Medicine we’ve pioneered a way to examine the AR pathway with a simple blood test.
To do this we use an extremely specialized technology that captures the very small fragments or rare circulating tumor cells on a “chip.” From this chip we are able to determine which cells are responding to treatment.
In real time, we can see taxane chemotherapy kept the (green) AR out of the (blue) nucleus area in cells from a responding patient.
In cancer care, we are always trying to maximize treatment response rates by targeting the right cells at the right time. This promising precision medicine approach offers us one more tool to better personalize treatment and improve outcomes.


 Dr. Scott Tagawa presented
Dr. Scott Tagawa presented